News
Elecsys® PIVKA-II

A sensitive and accurate tool for use as an aid in the diagnosis of HCC
What are the current limitations in current HCC surveillance methods?1
Only 63% Sensitivity2
of Ultrasound + AFP
in detecting early stage HCC
37%
will be missed

- Poor performance in patients with fibrotic changes and fatty infiltration of the liver
- Difficult to perform in obese patients
- Difficult to detect small lesions (< 2cm)
- Limited capacity in public hospitals and rural settings
- Operator variability

AFP is not specific for HCC. It can be elevated (false positive) in the following conditions:
- Cirrhosis
- Active hepatitis
- Other types of tumours
AFP can be normal (false negative) in the following conditions:
- Certain HCC patients have normal AFP throughout the entire disease course
- Small size HCC (tumour < 2 cm)
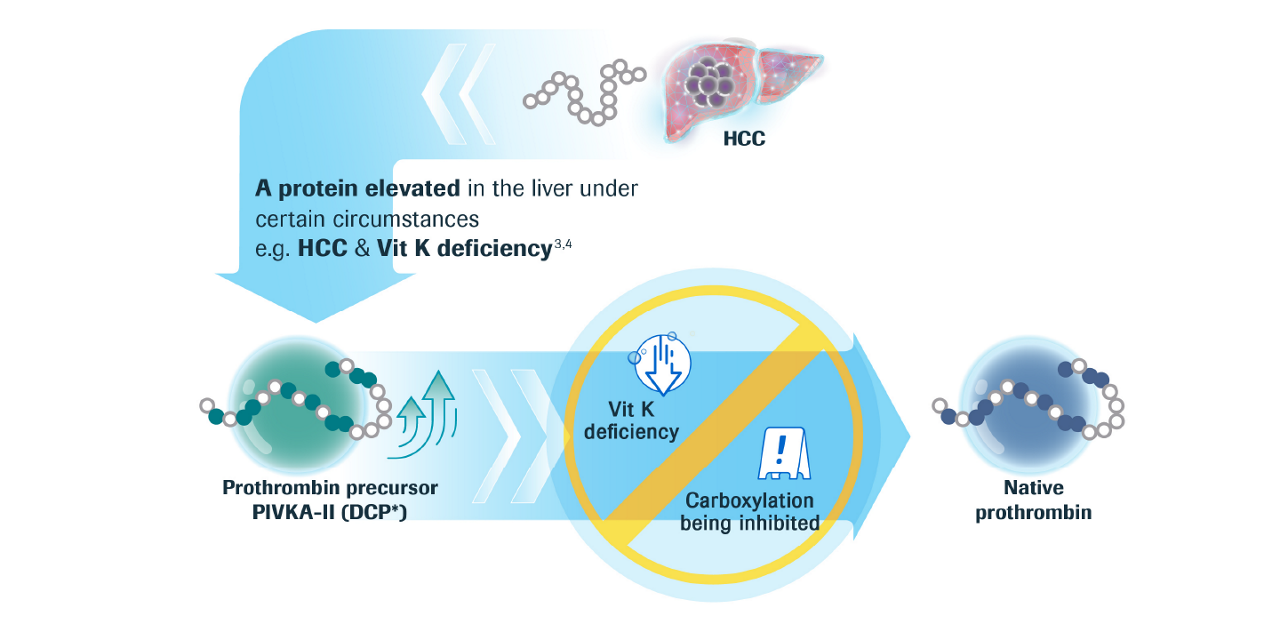
What is PIVKA-II?

PIVKA-II detects HCC with a higher sensitivity vs AFP5
Comparison between PIVKA-II and AFP
| All HCC | Early Stage HCC* | Late Stage HCC† | ||||
|---|---|---|---|---|---|---|
| Marker | PIVKA-II | AFP | PIVKA-II | AFP | PIVKA-II | AFP |
| Sensitivity (95% CI) |
86.90%(80.8%, 91.6%) |
51.80% (44%, 59.5%) |
77.90%(67%, 86.6%) |
36.40% (25.7%, 48.1%) |
94.50%(87.6%, 98.2%) |
64.80% (54.1%, 74.6%) |
Specificity |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
| ROC AUC§ | 90.80% (87.5%−94.1%) |
88% (84.5%−91.5% |
84.70% (78.7%−90.8%) |
84.50% (79.3%−89.7%) |
95.50% (93.2%−98.7%) |
90.90% (86.8%−95.1%) |
| All HCC | ||
|---|---|---|
| Marker | PIVKA-II | AFP |
| Sensitivity (95% CI) |
86.90%(80.8%, 91.6%) |
51.80% (44%, 59.5%) |
| Specificity (95% CI) |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
| ROC AUC§ | 90.80% (87.5%−94.1%) |
88% (84.5%−91.5%) |
| Early Stage HCC* | ||
|---|---|---|
| Marker | PIVKA-II | AFP |
| Sensitivity (95% CI) |
77.90%(67%, 86.6%) |
36.40% (25.7%, 48.1%) |
| Specificity (95% CI) |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
| ROC AUC§ | 84.70% (78.7%−90.8%) |
84.50% (79.3%−89.7%) |
| Late Stage HCC† | ||
|---|---|---|
| Marker | PIVKA-II | AFP |
| Sensitivity (95% CI) |
94.50%(87.6%, 98.2%) |
64.80% (54.1%, 74.6%) |
| Specificity (95% CI) |
83.70% (77.9%, 88.4%) |
98.10% (95.1%, 99.5%) |
| ROC AUC§ | 95.50% (93.2%−98.7%) |
90.90% (86.8%−95.1%) |
At the cut-off of 28.4 ng/mL Elecsys PIVKA-II shows a higher sensitivity
vs AFP surveillance cut-off of 20 ng/mL5,6
*BCLC stages 0, A † BCLC stages B,C,D ‡ Applies to sensitivity and specificity only § Area under the Curve
What is the best recommended approach for better and more accurate diagnosis?
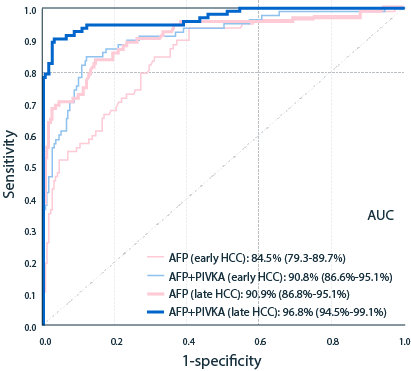
The combination of PIVKA-II and AFP
has markedly better sensitivity for detecting HCC vs AFP alone7
Comparison between PIVKA-II + AFP and AFP
| AFP | AFP + PIVKA-II | |
|---|---|---|
| Sensitivity (All HCC) |
51.8% | 91.7% |
| Sensitivity (Early Stage HCC)* |
36.4% | 87.0% |
| Specificity (Late Stage HCC)† |
64.8% | 95.6% |
| Specificity | 98.1% | 82.2% |
* BCLC stages 0, A; † BCLC stages B,C,D
| AFP | AFP + PIVKA-II | |
|---|---|---|
| Sensitivity (All HCC) |
51.8% | 91.7% |
| Sensitivity (Early Stage HCC)* |
36.4% | 87.0% |
| Specificity (Late Stage HCC)† |
64.8% | 95.6% |
| Specificity | 98.1% | 82.2% |
* BCLC stages 0, A; † BCLC stages B,C,D

By using the combination of PIVKA-II, AFP and US, we can improves the sensitivity for detection of HCC

By using the combination of PIVKA-II, AFP and US, we can improves the sensitivity for detection of HCC
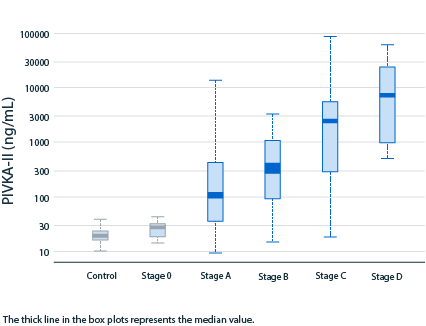
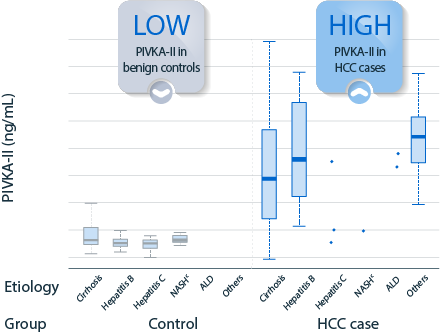
PIVKA-II concentration reliably shows gradual
HCC disease progression and clear differentiation5,7
Range of PIVKA-II distribution
PIVKA-II concentration and disease etiology
Useful Resources

Liver Experts for Advancement of HCC Care and Detection
Access to webinars recording for
update on biomarker in HCC
surveillance and treatment
Access to webinars recording for
update on biomarker in HCC
surveillance and treatment
...
References
- Simmons,O.etal.(2017),Predictorsofadequateultrasoundqualityforhepatocellularcarcinomasurveillanceinpatientswithcirrhosis.AlimentPharmacolTher,45:169-177.doi:10.1111/apt.13841; EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma., Journal of Hepatology, Volume 69, Issue 1, 2018, Pages 182-236, ISSN 0168-8278; Sherman M. Limitations of screening for hepatocellular carcinoma. Hepat Oncol. 2014;1(2):161–163. doi:10.2217/hep.13.22
- Singal, A.G.,et al.. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients With Cirrhosis: A Meta-analysis. Gastroenterology. 2018 May;154(6):1706-1718.e1.
- Liebmann, H.A. et al. (1984). Des-gamma-carboxy (abnormal) prothrombin as a serum marker of primary hepatocellular carcinoma. N Eng J Med 310, 1427-1431.
- Ono, M. et al. (1990). Measurement of immunoreactive prothrombin precursor and vitamin-K-dependent gamma-carboxylation in human hepatocellular carcinoma tissues: Decreased carboxylation of prothrombin precursor as a cause of des-gamma-carboxy prothrombin synthesis. Tumour Biol 11, 319-326.
- Chan, H. L. Y., Vogel, A., Berg, T., De Toni, E. N., Kudo, M., Trojan, J., ... & Piratvisuth, T. (2020, November). ELECSYS PIVKA-II AND ELECSYS AFP ASSAYS DEMONSTRATE GOOD CLINICAL PERFORMANCE FOR HEPATOCELLULAR CARCINOMA (HCC) DIAGNOSIS ACROSS DIFFERENT DISEASE STAGES AND ETIOLOGIES. In The Liver Meeting Digital Experience™. AASLD.
- Chang TS et al. Am J Gastroenterol 2015;110:836–844
- Roche CE method sheet PIVKA-II 2020 (Roche studies No. RD002542 and RD002543)
MAP-2023-JUL-002