
Elecsys® Anti‑SARS‑CoV‑2 S for use on the cobas e analyzers is an electrochemiluminescence immunoassay intended for qualitative and semi-quantitative detection of antibodies to SARS‑CoV‑2 spike (S) protein receptor binding domain (RBD) in human serum and plasma (lithium heparin, dipotassium-EDTA, tripotassium-EDTA, and sodium citrate). The Elecsys Anti‑SARS‑CoV‑2 S assay is intended as an aid in identifying individuals with an adaptive immune response to SARS‑CoV‑2, indicating recent or prior infection. The Elecsys Anti‑SARS‑CoV‑2 S assay should not be used to diagnose or exclude acute SARS‑CoV‑2 infection.
Elecsys® Anti-SARS-CoV-2 S
Immunoassay for the qualitative and semi-quantitative determination of antibodies to the SARS-CoV-2 spike protein. For use under the Emergency Use Authorization (EUA) only.
IVD
For in vitro diagnostic use.

Immunoassay for the semi-quantitative determination of antibodies to the SARS-CoV-2 spike protein
SARS-CoV-2: An overview of virus structure, transmission and detection
SARS-CoV-2, the causative agent of Coronavirus Disease 2019 (COVID-19), is an enveloped, single-stranded RNA Betacoronavirus. Seven coronaviruses have been identified as agents of human infection, causing disease ranging from mild common cold to severe respiratory failure.1
SARS-CoV-2 is transmitted primarily from person-to-person through respiratory droplets and aerosols.2,3 The incubation period from infection to detectable viral load in the host commonly ranges from two to 14 days.4,5 Detection of viral load can be associated with the onset of clinical signs and symptoms, although a considerable proportion of individuals remain asymptomatic or mildly symptomatic.6-8 The interval during which an individual with COVID-19 is infectious has not yet been clearly established, however, transmission from symptomatic, asymptomatic, and pre-symptomatic individuals has been well described.9-11
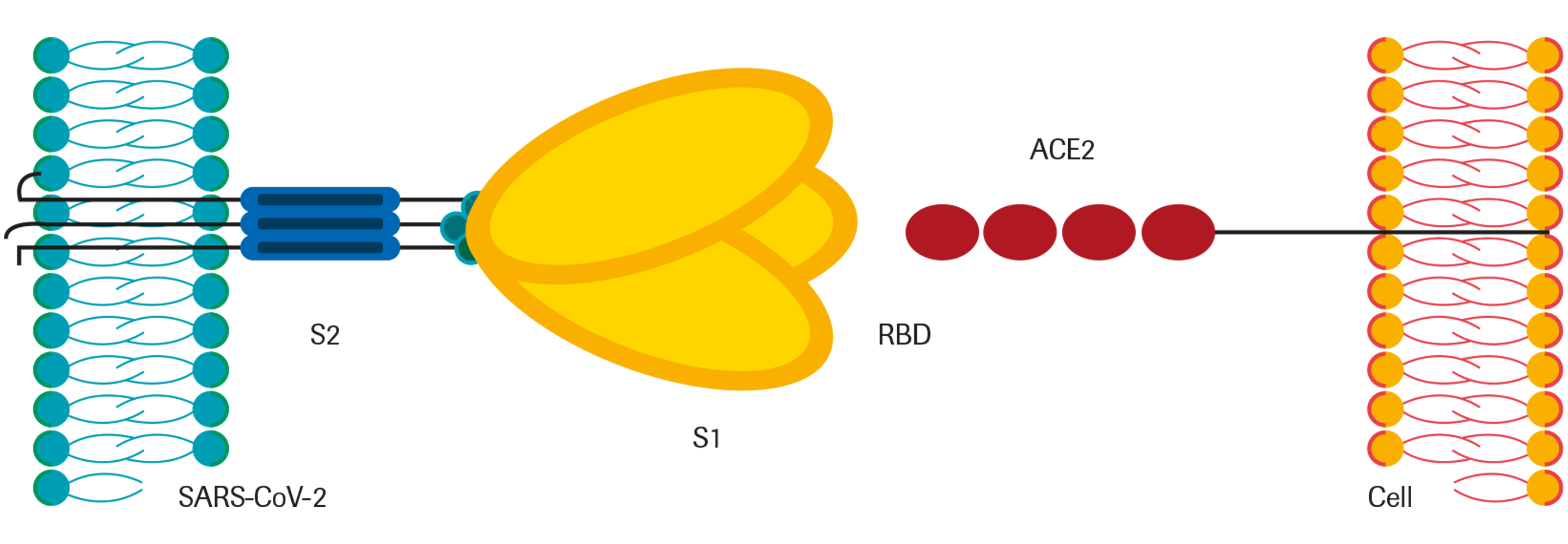
Coronavirus genomes encode 4 main structural proteins: spike (S), envelope (E), membrane (M), and nucleocapsid (N). The S protein is a very large transmembrane protein that assembles into trimers to form the distinctive surface spikes of coronaviruses. Each S monomer consists of an N-terminal S1 subunit and a membrane-proximal S2 subunit. The virus gains entry to the host cell through binding of the S protein to the angiotensin-converting enzyme 2 (ACE2) receptor, which is present on the surface of numerous cell types including the alveolar type II cells of the lung and epithelial cells of the oral mucosa.12,13 Mechanistically, ACE2 is engaged by the receptor-binding domain (RBD) on the S1 subunit.14,15
Upon infection with SARS-CoV-2, the host usually mounts an immune response against the virus, typically including production of specific antibodies against viral antigens. IgM and IgG antibodies against SARS-CoV-2 appear to arise nearly simultaneously in blood.16 There is significant inter-individual difference in the levels and chronological appearance of antibodies in COVID-19 patients, but median seroconversion has been observed at approximately two weeks.17-20
After infection or vaccination, the binding strength of antibodies to antigens increases over time - a process called affinity maturation21. High‑affinity antibodies can elicit neutralization by recognizing and binding specific viral epitopes22,23. Antibodies against SARS‑CoV‑2 with strong neutralizing capacity, especially potent if directed against the RBD, have been identified.24-27 Numerous vaccines for COVID-19 are in development, many of which focus on eliciting an immune response to the RBD.28-30
Structure of the SARS-CoV-2 spike protein and binding to host receptor
Positive Percent Agreement
View full tablePositive Percent Agreement
A total of 1485 samples from 331 symptomatic patients (including
172 samples from 172 hospitalized patients) with a PCR confirmed
SARS‑CoV‑2 infection were tested with the Elecsys Anti‑SARS‑CoV‑2 S
assay. 1 or more sequential samples from these patients were collected at
various time points after PCR confirmation. Positive percent agreement
(PPA) was correlated with days post PCR specimen collection, and the
results are shown for the first bleed per time bin.
First bleed
233 of the tested samples had a sampling date of 15 days or later after
diagnosis with PCR. 225 of these 233 samples were determined with
≥ 0.8 U/mL in the Elecsys Anti‑SARS‑CoV‑2 S assay and hence considered
positive, resulting in a PPA of 96.6 % (95 % CI: 93.35‑98.51 %) in this
sample cohort.
A total of 1485 samples from 331 symptomatic patients (including
172 samples from 172 hospitalized patients) with a PCR confirmed
SARS‑CoV‑2 infection were tested with the Elecsys Anti‑SARS‑CoV‑2 S
assay. 1 or more sequential samples from these patients were collected at
various time points after PCR confirmation. Positive percent agreement
(PPA) was correlated with days post PCR specimen collection, and the
results are shown for the first bleed per time bin.
First bleed
233 of the tested samples had a sampling date of 15 days or later after
diagnosis with PCR. 225 of these 233 samples were determined with
≥ 0.8 U/mL in the Elecsys Anti‑SARS‑CoV‑2 S assay and hence considered
positive, resulting in a PPA of 96.6 % (95 % CI: 93.35‑98.51 %) in this
sample cohort.
| Days after PCR positive result | Number tested | Pos | Neg | PPA (%) | 95 % CI* (%) |
| 0-7 | 32 | 29 | 3 | 90.6 | (74.9 - 98.0) |
| 8-14 | 77 | 67 | 10 | 87.0 | (77.4 - 93.5) |
| ≥ 15 | 233 | 225 | 8 | 96.6 | (93.3 - 98.5) |
Analytical specificity 31
View full tableAnalytical specificity 31
A total of 1,468 potentially cross-reactive samples collected before October 2019, including anti-MERS-CoV positive samples, samples from individuals with common cold symptoms, and samples from individuals confirmed to be infected with one of the four common cold coronaviruses were tested with the Elecsys® Anti-SARS-CoV-2 S assay. Overall specificity in this cohort of potentially cross-reactive samples was 100 % (95 % CI: 99.7 – 100 %).
A total of 1,468 potentially cross-reactive samples collected before October 2019, including anti-MERS-CoV positive samples, samples from individuals with common cold symptoms, and samples from individuals confirmed to be infected with one of the four common cold coronaviruses were tested with the Elecsys® Anti-SARS-CoV-2 S assay. Overall specificity in this cohort of potentially cross-reactive samples was 100 % (95 % CI: 99.7 – 100 %).
| Cohort | N | Reactive | Specificity (95% CI) |
| MERS-CoV* | 51 | 0 | 100 % |
| Common cold panel** | 21 | 0 | 100 % |
| Common Coronavirus panel*** | 151 | 0 | 100 % |
| Other potentially cross-reactive samples**** | 978 | 0 | 100 % |
| Overall | 1,468 | 0 | 100 % |
** 40 samples from individuals with common cold symptoms, collected before October 2019
*** from individuals with past infection with coronavirus HKU1, NL63, 229E, or OC43, confirmed by antigen testing
**** pre-pandemic samples with reactivity for various other indications, which could have an elevated potential for unspecific interference
Negative Percent Agreement 31
View full tableNegative Percent Agreement 31
A total of 5,991 samples from diagnostic routine and blood donors drawn before October 2019 were tested with the Elecsys® Anti-SARSCoV-2 S assay. Overall Negative Percent Agreement (NPA) in this cohort of pre-pandemic samples was 99.98 % (95 % CI: 99.91 – 100 %).
A total of 5,991 samples from diagnostic routine and blood donors drawn before October 2019 were tested with the Elecsys® Anti-SARSCoV-2 S assay. Overall Negative Percent Agreement (NPA) in this cohort of pre-pandemic samples was 99.98 % (95 % CI: 99.91 – 100 %).
| Cohort | N | Reactive | NPA (95 % CI) |
| Diagnostic routine | 2,528 | 0 | 100 % (99.8 – 100 %) |
| US blood donors | 2,713 | 1 | 99.9 % (99.7 – 100 %) |
| African blood donors | 750 | 0 | 100 % (99.5 – 100 %) |
| Overall | 5,991 | 1 | 99.9 % (99.9 – 100 %) |
Estimated course of markers in SARS-CoV-2 infection33
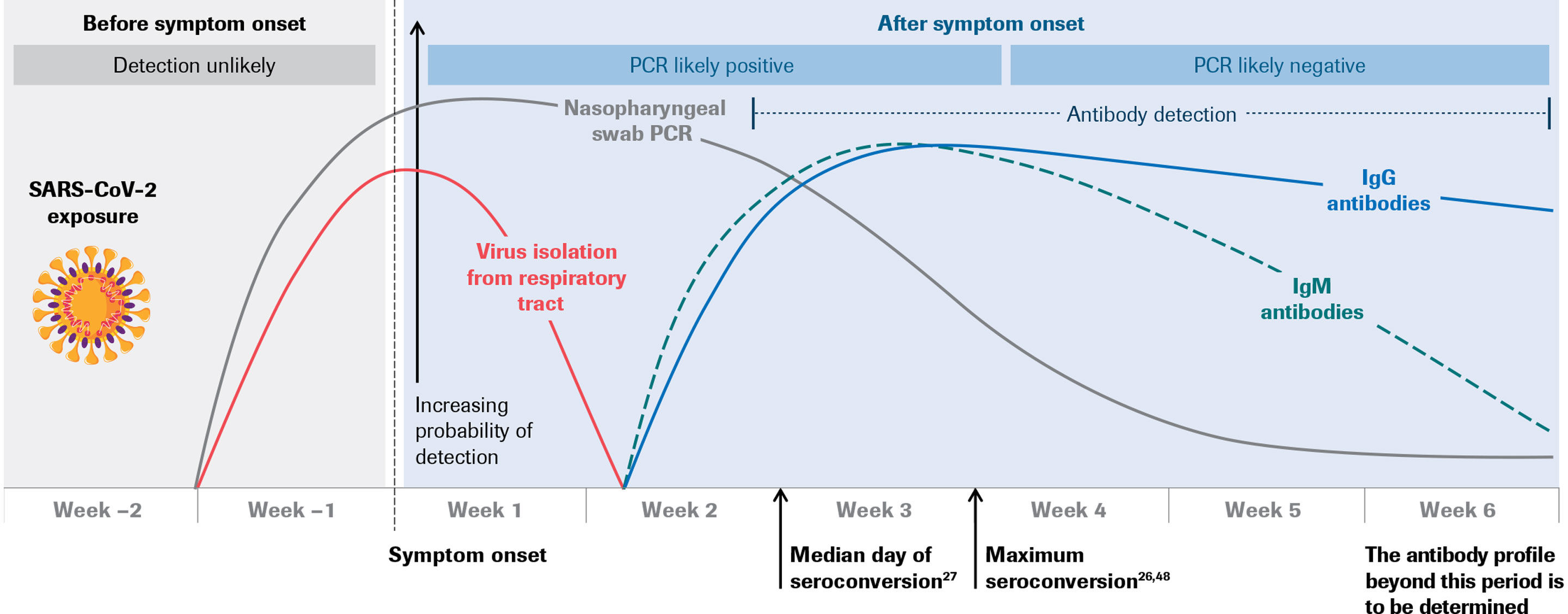
Estimated course of markers in SARS-CoV-2 infection47
WARNING:
For use under Emergency Use Authorization only. This test has not been FDA-cleared or ‑approved; this test has been authorized by FDA under an Emergency Use Authorization (EUA) for use by authorized laboratories; by laboratories certified under the Clinical Laboratory Improvement Amendments of 1988 (CLIA), 42 U.S.C. 263a, that meet requirements to perform high complexity tests. This test has been authorized only for detecting antibodies against SARS‑CoV‑2, not for any other viruses or pathogens. This test is only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of in vitro diagnostic tests for detection and/or diagnosis of COVID‑19 under Section 564(b)(1) of the Federal Food, Drug, and Cosmetic Act, 21 U.S.C § 360bbb‑3(b)(1), unless the authorization is terminated or revoked sooner.
References
- Ye, Z.-W. (2020). Int J Biol Sci. 16(10), 1686-97.
- Word Health Organization (2020). Available from: https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions.
- Zhu, N. et al. (2020). N Engl J Med. 20, 382(8), 727-33.
- Chan, J.F.-W. et al. (2020). Lancet. 15, 395(10223), 514-23.
- Lauer, S.A. et al. (2020). Ann Intern Med. 172(9), 577-582.
- Zhou, R. et al. (2020). Int J Inf Dis. 96, 288-90.
- He, X. et al. (2020). Nat Med. 26(5), 672-5.
- Mizumoto, K. et al. (2020). Euro Surveill. 25(10), pii=2000180.
- Gao, M. et al. (2020). Respir Med. 169, 106026.
- Yu, P. et al. (2020). J Infect Dis. 221(11), 1757-61.
- Liu, Z. et al. (2020). Int J Inf Dis. https://doi.org/10.1016/j.ijid.2020.06.036.
- Letko, M. et al. (2020). Nat Microbiol. 5(4), 562-9.
- Xu, H. et al. (2020). Int J Oral Sci. 24, 12(1), 1-5.
- Wrapp, D. et al. (2020). Science. 13, 367(6483), 1260-3.
- Hoffmann, M. et al. (2020). Cell. 16, 181(2), 271-280.e8.
- Centers for Disease Control and Prevention (2020). Available from: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html.
- Long, Q. et al. (2020). medRxiv. https://doi.org/10.1101/2020.03.18.20038018.
- Lou, B. et al. (2020). Eur Respir J. 19, 2000763.
- Zhao, J. et al. Clin Infect Dis. ciaa344. https://doi.org/10.1093/cid/ciaa344.
- Tuaillon, E. et al. (2020). J Inf. 81(2), e39-e45.
- Klasse, P.J. (2016). Expert Rev Vaccines 15(3), 295-311.
- Payne, S. (2017). Viruses: Chapter 6 – Immunity and Resistance to Viruses, Editor(s): Susan Payne, Academic Press, Pages 61-71, ISBN 9780128031094.
- Iwasaki, A. and Yang, Y. (2020). Nat Rev Immunol. https://doi.org/10.1038/s41577-020-0321-6.
- Salazar, E. et al. (2020). bioRxiv 2020.06.08.138990; https://doi.org/10.1101/2020.06.08.138990.
- Klasse, P. and Moore, J.P. (2020). Elife. 2020, 9:e57877. doi:10.7554/eLife.57877.
- Premkumar, L. et al. (2020). Sci Immunol. 11, 5(48).
- Luchsinger, L.L. et al. (2020). medRxiv. https://doi.org/10.1101/2020.06.08.20124792
- Mukherjee, R. (2020). J Biosci. 45, 68. https://doi.org/10.1007/s12038-020-00040-7.
- Graham, B.S. (2020). Science. 368(6494), 945-6.
- Hotez, P.J. et al. (2020). Nat Rev Immunol. 20(6), 347-8.
- Elecsys Anti-SARS-CoV-2 S. Package Insert 2022-03, V3.0; Material Numbers 09289267190 and 09289275190.
- Meyer, B. et al. medRxiv. https://doi.org/10.1101/2020.05.02.20080879.
- Sethuraman, N. et al. (2020). JAMA. Published online May 06, 2020. doi:10.1001/jama.2020.8259.
- To, K. et al. (2020). Lancet Infect Dis. 20(5), 565-74.
- Xiang, F. et al. (2020). Clin Infect Dis. pii: ciaa46. https://doi.org/10.1093/cid/ciaa461.
Use left and right arrow keys to scroll between the tabs
