
Elecsys® Anti-SARS-CoV-2 is an immunoassay intended for the qualitative detection of antibodies to SARS-CoV-2 in human serum and plasma. The assay uses a recombinant protein representing the nucleocapsid (N) antigen for the determination of antibodies against SARS-CoV-2. The test is intended for use as an aid in identifying individuals with an adaptive immune response to SARS-CoV-2, indicating recent or prior infection.43
Elecsys® Anti-SARS-CoV-2
Immunoassay intended for qualitative detection of antibodies to SARS-CoV-2 in human serum and plasma.
For use under the Emergency Use Authorization (EUA) only.
For use under the Emergency Use Authorization (EUA) only.
IVD
For in vitro diagnostic use.

Immunoassay to qualitatively detect antibodies against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)
SARS-CoV-2: An overview of virus structure, transmission and detection
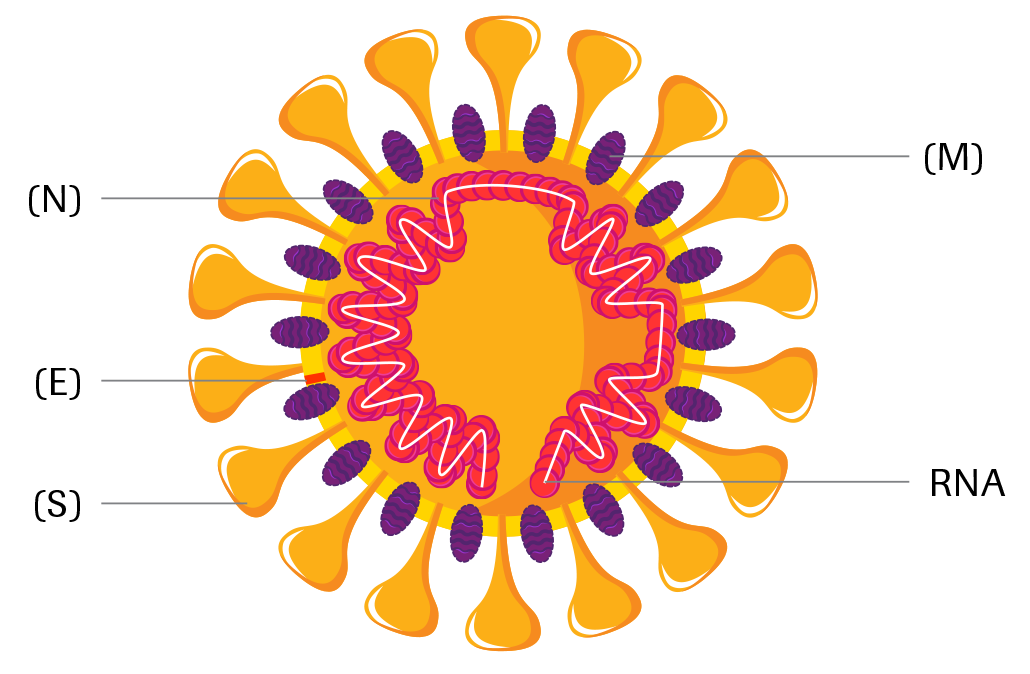
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is an enveloped, single-stranded RNA virus of the family Coronaviridae. Coronaviruses share structural similarities and are composed of 16 nonstructural proteins and 4 structural proteins: spike (S), envelope (E), membrane (M), and nucleocapsid (N). Coronaviruses cause diseases with symptoms ranging from those of a mild common cold to more severe ones such as Coronavirus Disease 2019 (COVID-19) caused by SARS-CoV-2 1,2.
SARS-CoV-2 is transmitted from person-to-person primarily via respiratory droplets, while indirect transmission through contaminated surfaces is also possible3-6. The virus accesses host cells via the angiotensin-converting enzyme 2 (ACE2), which is most abundant in the lungs7,8.
The incubation period for COVID-19 ranges from 2 – 14 days following exposure, with most cases showing symptoms approximately 4 – 5 days after exposure3,9,10. The spectrum of symptomatic infection ranges from mild (fever, cough, fatigue, loss of smell and taste, shortness of breath) to critical11,12. While most symptomatic cases are not severe, severe illness occurs predominantly in adults with advanced age or underlying medical comorbidities and requires intensive care. Acute respiratory distress syndrome (ARDS) is a major complication in patients with severe disease. Critical cases are characterized by e.g., respiratory failure, shock and/or multiple organ dysfunction, or failure11,13,14.
Definite COVID-19 diagnosis entails direct detection of SARS-CoV-2 RNA by nucleic acid amplification technology (NAAT)21-23. Serological assays, which detect antibodies against SARS-CoV-2, can contribute to identify individuals, which were previously infected by the virus, and to assess the extent of exposure of a population. They might thereby help to decide on application, enforcement or relaxation of containment measures24.
Upon infection with SARS-CoV-2, the host mounts an immune response against the virus, including production of specific antibodies against viral antigens. Both IgM and IgG have been detected as early as day 5 after symptom onset25,26. Median seroconversion has been observed at day 10 – 13 for IgM and day 12 – 14 for IgG27-29, while maximum levels have been reported at week 2 – 3 for IgM, week 3 – 6 for IgG and week 2 for total antibody25-31. Whereas IgM seems to vanish around week 6 – 732,33, high IgG seropositivity is seen at that time25,32,33. While IgM is typically the major antibody class secreted to blood in the early stages of a primary antibody response, levels and chronological order of IgM and IgG antibody appearance seem to be highly variable for SARS-CoV-2. Anti-SARS-CoV-2 IgM and IgG often appear simultaneously, and some cases have been reported where IgG appears before IgM, limiting its diagnostic utility26,27,29,34,35.
After infection or vaccination, the binding strength of antibodies to antigens increases over time – a process called affinity maturation36. High-affinity antibodies can elicit neutralization by recognizing and binding specific viral epitopes37,38. In SARS-CoV-2 infection, antibodies targeting both the spike and nucleocapsid proteins, which correlate with a strong neutralizing response, are formed as early as day 9 onwards, suggesting seroconversion may lead to protection for at least a limited time34,39-42.
Structure of the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)
- Nucleocapsid protein (N)
- Envelope protein (E)
- Spike protein (S)
- Membrane glycoprotein (M)
- RNA
Estimated course of markers in SARS-CoV-2 infection44

* COI: cutoff index
Clinical specificity43
View full tableClinical specificity43
A total of 10,453 samples from diagnostic routine and blood donors obtained before December 2019 were tested with the Elecsys® Anti-SARS-CoV-2 assay.
A total of 10,453 samples from diagnostic routine and blood donors obtained before December 2019 were tested with the Elecsys® Anti-SARS-CoV-2 assay.
| Cohort | N | Reactive | Specificity % (95 % CI) |
| Diagnostic routine | 6305 | 12 | 99.81 % (99.67 – 99.90 %) |
| Blood donors | 4148 | 9 | 99.78 % (99.59 – 99.90 %) |
| Overall | 10453 | 21 | 99.80 % (99.69 – 99.88 %) |
|---|
Analytical specificity43
Overall specificity in a cohort of 792 potentially cross-reactive samples was 99.5 % (95 % CI: 98.63 – 99.85 %).
* 40 samples from individuals with common cold symptoms, collected before Dec 2019
** 40 samples from individuals following an infection with Coronavirus HKU1, NL63, 229E or OC43, confirmed by PCR
*** N=712
Common cold panel*
100 % specificity
Coronavirus panel**
100 % specificity
Other potential cross-reactivity***
99.44 % specificity
Clinical sensitivity43
View full tableClinical sensitivity43
A total of 496 samples from 102 symptomatic patients with a PCR confirmed SARS-CoV-2 infection were tested with the Elecsys® Anti-SARS-CoV-2 assay. One or more sequential specimens from these patients were collected after PCR confirmation at various time points.
A total of 496 samples from 102 symptomatic patients with a PCR confirmed SARS-CoV-2 infection were tested with the Elecsys® Anti-SARS-CoV-2 assay. One or more sequential specimens from these patients were collected after PCR confirmation at various time points.
| Days post PCR confirmation | N | Non-reactive | Sensitivity (95 % CI**) |
| 0 – 6 days | 161 | 64 | 60.2 % (52.3 – 67.8 %) |
| 7 – 13 days | 150 | 22 | 85.3 % (78.6 – 90.6 %) |
| ≥14 days | 185 | 1* | 99.5 % (97.0 – 100 %) |
Seroconversion sensitivity43
After recovery from infection, confirmed by a negative PCR result, 26 consecutive samples from 5 individuals were tested with the Elecsys® Anti-SARS-CoV-2 assay.

* Day 0 represents initial positive PCR
Testing modules

cobas e 801 module
- Throughput of up to 300 tests/hour
- 48 reagent positions
Part of the cobas 8000 modular analyzer series and cobas pro integrated solutions.

cobas e 602 module
- Throughput of up to 170 tests/hour
- 25 reagent positions
Part of the cobas 8000 modular analyzer series.

cobas e 601 module
- Throughput of up to 170 tests/hour
- 25 reagent positions
Part of the cobas 6000 modular analyzer series.

cobas e 411 analyzer
- Up to 86 tests/hour
- Benchtop
Part of the cobas 4000 modular analyzer series.
WARNING:
- This test has not been FDA cleared or approved.
- Not for screening of donated blood.
- This test has been authorized by FDA under an EUA for use by authorized laboratories.
- This test has been authorized only for detecting the presence of antibodies against SARS-CoV-2, not for any other viruses or pathogens.
- This test is only authorized for the duration of the declaration that circumstances exist justifying the authorization of emergency use of in vitro diagnostics for detection and/or diagnosis of COVID-19 under Section 564(b)(1) of the Act, 21 U.S.C. § 360bbb-3(b)(1), unless the authorization is terminated or revoked sooner.
References
- Su, S. et al. (2016). Trends Microbiol. 24(6), 490-502.
- Zhu, N. et al. (2020). N Engl J Med. 382(8), 727-733.
- Chan, J.F. et al. (2020). Lancet. 395, 514-523.
- U.S. CDC. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html. Published April 2, 2020. Accessed April 15, 2020.
- WHO. https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations. Published March 29, 2020. Accessed April 15, 2020.
- Kampf, G. et al. (2020). J Hosp Infect. 104(3), 246-251.
- Letko, M. et al. (2020). Nat Microbiol. 5, 562-5.
- Hoffmann, M. et al. (2020). Cell. 181, 271-80.e8.
- WHO. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200403- sitrep-74-covid-19-mp.pdf. Published April 3, 2020. Accessed April 15, 2020.
- Lauer, S.A. et al. (2020). Ann Intern Med. 172(9), 577-82.
- Rothe, C. et al. (2020). N Engl J Med. 382(10), 970-971.
- Kupferschmidt, K. Study claiming new coronavirus can be transmitted by people without symptoms was flawed. Science. https://www.sciencemag.org/news/2020/02/paper-non-symptomatic-patient-transmitting-coronavirus-wrong. Published February 4, 2020. Accessed April 15, 2020.
- Bai, Y. et al. (2020). JAMA. 323(14), 1406-1407.
- Mizumoto, K. et al. (2020). Euro Surveill. 25(10), 2000180.
- Hu, Z. et al. (2020). Sci China Life Sci. 63(5), 706-711.
- U.S. CDC. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. Published March 20, 2020. Accessed April 15, 2020.
- Wang, D. et al. (2020). JAMA. 323(11), 1061-1069.
- Huang, C. et al. (2020). Lancet. 395(10223), 15-2.
- Arentz, M. et al. (2020). JAMA. 323(16), 1612-1614.
- Wu, Z. et al. JAMA. 323(13), 1239-1242.
- WHO. https://apps.who.int/iris/bitstream/handle/10665/331501/WHO-COVID-19- laboratory-2020.5-eng.pdf. Published March 19, 2020. Accessed April 15, 2020.
- U.S. CDC. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-criteria.html. Published March 14, 2020. Accessed April 15, 2020.
- EUCDC. https://www.ecdc.europa.eu/sites/default/files/documents/Overview-rapid-test-situation-for-COVID-19-diagnosis-EU-EEA.pdf. Published April 1, 2020. Accessed April 15, 2020.
- WHO. https://www.who.int/blueprint/priority-diseases/key-action/novel-coronavirus/en/. Published April 11, 2020. Accessed April 15, 2020.
- Liu, W. et al. (2020). J Clin Microbiol. 58(6), e00461-2.
- To, K. et al. (2020). Lancet Infect Dis. 20(5), 565-74.
- Long, Q. et al. (2020). medRxiv. https://doi.org/10.1101/2020.03.18.20038018.
- Lou, B. et al. (2020). Eur Resp J. https://doi.org/10.1183/13993003.00763-2020.
- Zhao, J. et al. (2020). Clin Infect Dis. pii: ciaa344. https://doi.org/10.1093/cid/ciaa344.
- Zhang, B. et al. (2020). medRxiv. https://doi.org/10.1101/2020.03.12.20035048.
- Wölfel, R. et al. (2020). Nature. 581, 465-469.
- Xiao, D.A.T. et al. (2020). J Infect. 81(1), 147-178.
- Tan, W. et al. (2020). medRxiv. https://doi.org/10.1101/2020.03.24.20042382.
- Okba, N. et al. (2020). medRxiv. https://doi.org/10.1101/2020.03.18.20038059.
- Alberts, B. et al. (2002). Molecular Biology of the Cell. 4th edition. New York: Garland Science. B Cells and Antibodies. Available from: https://www.ncbi.nlm.nih.gov/books/NBK26884/
- Klasse, P.J. (2016). Expert Rev Vaccines 15(3), 295-311.
- Payne, S. (2017). Viruses: Chapter 6 - Immunity and Resistance to Viruses, Editor(s): Susan Payne, Academic Press, Pages 61-71, ISBN 9780128031094.
- Iwasaki, A. and Yang, Y. (2020). Nat Rev Immunol. https://doi.org/10.1038/ s41577-020-0321-6.
- Amanat, F. et al. (2020). Nat Med. https://doi.org/10.1038/s41591-020-0913-5.
- Zhou, P. et al. (2020). Nature. 579(7798), 270-273.
- Haveri, A. et al. (2020). Euro Surveill. 25(11), 2000266.
- Poh, C. et al. (2020). bioRxiv. preprint doi: https://doi.org/10.1101/2020.03.30.015461.
- Elecsys® Anti-SARS-CoV-2. Package Insert 2020-07, V4.0; Material Numbers 09203095190 and 09203079190.
- Sethuraman, N. et al. (2020). JAMA. Published online May 06, 2020. doi:10.1001/jama.2020.8259.
- Xiang, F. et al. (2020). Clin Infect Dis. pii: ciaa46. doi:10.1093/cid/ciaa461.
Use left and right arrow keys to scroll between the tabs
