Breast cancer IHC/ISH portfolio

It’s why we do what we do.
Together with our partners, we’re committed to improving outcomes by providing the most comprehensive diagnostic tools that enable you to confidently deliver personalized results for every patient.
Our commitment to treating breast cancer includes over 25 assays, which can help accurately determine the tumor lineage and identify unsegmented patient populations that can help clinicians identify appropriate treatment options.
Why is this so important to us?
Because breast cancer is the most common cancer among women.



Every breast tissue sample received in the lab represents someone’s life. A life that deserves a swift, accurate diagnosis and treatment. Our tests focus on accurate results to help clinician care teams determine a patient’s personalized treatment path.
HER2-IHC

HER2 Dual ISH

Cornerstone Assays

Going further for breast cancer patients. Driving diagnostic certainty.
Breast cancer is a deeply personal experience that’s different for every patient. That’s why it’s so important to determine the type of breast cancer, and in turn, the right treatment path.
Since 1991, Roche Tissue Diagnostics has battled cancer with innovation. This comes in the form of the most comprehensive panel of advanced diagnostic tools that have the potential to profoundly change, and hopefully save, lives.
Clinical utility, superior specificity and sensitivity, and testing efficiency work together to create the big picture and ultimately our why—improved time to treatment for the patient.
Would you like to know more about our Breast cancer IHC/ISH portfolio?
Please submit your information in the following form to be contacted by a Roche representative with more details.

Let’s start with clinical utility.
The Roche Breast Cancer Diagnostics Portfolio solution provides you with all of the diagnostic assays and FDA-approved companion diagnostic biomarkers clinicians and patients need in the shortest possible time, quickly and reliably.

Superior specificity and sensitivity help you diagnose precisely and confidently.
Specific and sensitive rabbit monoclonal antibodies, best-in-class probes, and powerful detection systems help you diagnose precisely and confidently.

The benefits of testing efficiency reach far and wide.
Our comprehensive breast cancer portfolio delivers fully automated assays on market-leading platforms, with digital pathology and workflow solutions that reduce labor costs, free up resources, and improve time to results.

Pathology Lab product catalog
View our Pathology Lab product catalog to see our complete portfolio, including the many ways Roche supports customers.
References
PATHWAY anti-HER2/neu (4B5) Rabbit Monoclonal Primary Antibody Identifying HER2-low and HER2-ultralow expression
NOW FDA-approved for patients with HER2-ultralow levels of expression who may benefit from targeted treatment

Innovations in HER2-directed testing options deliver clear, confident results
First and only FDA-approved companion diagnostic for HER2/neu including HER2-low and HER2-ultralow expression
PATHWAY anti-HER2/neu (4B5) Rabbit Monoclonal Primary Antibody is the only FDA-approved CDx for HER2-low and ultralow expression. It’s FDA approved as a companion diagnostic for the breakthrough designated therapy ENHERTU®* (fam-trastuzumab deruxtecan-nxki). It’s the first and only test to identify metastatic breast cancer (mBC) patients with low and ultralow expression of HER2 who may be eligible for targeted therapy.
*For more information on ENHURTU® please refer to the FDA-approved product labeling.
PATHWAY anti-HER2/neu (4B5) is a registered trademark of Roche Diagnostics.
Advancements in diagnostic testing give hope to your mBC patients with low and ultralow levels of HER2 expression
Previously, there were no HER2-directed treatment options for the more than 50 percent of patients with mBC who were considered HER2-negative.
Thanks to advances in drug development targeting lower ranges of HER2 expression and the diagnostic innovation of Roche, these patients may qualify for personalized treatment that could potentially lead to improved outcomes.
HER2-low and ultralow are clinically significant sub-groups of HER2 expression1,2
100% of breast cancers tested for HER2

HER2-low FAQ—A Pathologist’s Perspective
Listen as Jim Richter, MD, Pathology Liaison within the Medical & Scientific Affairs division at Roche Diagnostics Corporation, provides insights on HER2-low from the pathologist’s perspective. He examines what HER2-low is, assessment/scoring, interpretation of tumor samples, related clinical trials, FDA approvals, patient care and safety, and so much more.
Discover how we’re going FURTHER.
To read our FAQs, please click here.
Indication for use: Breast cancer
View full tableIndication for use: Breast cancer
| Staining Pattern | HER2 Status | HER2 (4B5) Score (Report to treating physician) |
Clinical Application |
| No membrane staining is observed* | HER2-null | IHC 0 absent membrane staining | NONE |
| Any staining of the membrane in greater than 0 and less than or equal to 10% of the cancer cells*,**,*** | HER2-ultralow expression | IHC 0 with membrane staining | ENHERTU® (fam-trastuzumab deruxtecan-nxki) |
| Faint, partial staining of the membrane in greater than 10% of the cancer cells* | HER2-low expression | IHC 1+ | |
| Weak to moderate complete staining of the membrane in greater than 10% of the cancer cells | HER2-low expression | IHC 2+**** Reflex Test: HER2 non-amplified |
|
| HER2 positive / overexpression | IHC 2+**** Reflex Test: HER2 amplified |
HERCEPTIN® (trastuzumab), KADCYLA® (ado-trastuzumab emtansine) |
|
| Intense complete staining of the membrane in greater than 10% of the cancer cells | HER2 positive / overexpression | IHC 3+ |
**Recommend re-reading by a second pathologist for cases with “faint, partial staining of the membrane” and %TC ≤ 5%
*** In the HER2-ultralow “IHC 0 with membrane staining” category, partial membranous staining is usually faint but may exhibit stronger intensities, and such rare cases are scored as HER2-ultralow if they do not otherwise qualify for a higher score. Examples are shown in the case image section. Challenging cases as well as unusual staining patterns are provided for reference.
****Recommend reflex test to assess gene amplification per ASCO/CAP guidance
A breakthrough in diagnostic testing is helping to improve outcomes for patients like Enisa, who are receiving new targeted treatment for HER2-low breast cancer.
Learn more about Enisa’s journey and how Roche helps women fight breast cancer.
Confidently navigate the complexities of HER2 immunohistochemistry (IHC) testing in breast cancer
View this webinar to learn more about scoring and clinical significance of the newest companion diagnostic indication of PATHWAY anti-HER2 (4B5) for HER2-low.
Pathology Lab product catalog
View our Pathology Lab product catalog to see our complete portfolio, including the many ways Roche supports customers.
Reference
- PATHWAY HER2/neu Rabbit Monoclonal Antibody Method Sheet 14427us Rev K 2025-01-29.
VENTANA HER2 Dual ISH DNA Probe Cocktail assay

Together, we can advance personalized healthcare with companion diagnostics
We do this by giving you diagnostic confidence from a broad menu of clinically relevant predictive assays. Our standardized, fully automated, and easy-to-use solutions enable rapid turnaround time, empowering physicians to make the right patient treatment decisions more quickly.
Going further for patients with breast cancer through innovation
Based on input from pathologists and lab professionals like you, Roche created the VENTANA HER2 Dual ISH Probe Cocktail assay as part of the Roche Tissue Diagnostics Breast Cancer IHC/ISH Portfolio.

FDA approved as an aid in the assessment of patients for whom HERCEPTIN®* (trastuzumab) is being considered

Designed to improve turnaround time and first pass rates for confident results on the first read

Designed with brightfield technology for high-quality in-house testing
*For more information on HERCEPTIN® please refer to the FDA-approved product labeling.
Optimized with oligo probes, the VENTANA HER2 Dual ISH assay delivers clear, confident results
The VENTANA HER2 Dual ISH Probe Cocktail is a fully automated, ready-to-use brightfield solution for determining HER2 gene amplification. VENTANA HER2 Dual ISH helps identify breast cancer patients eligible for treatment with HERCEPTIN® (trastuzumab).

Bringing HER2 breast cancer testing in-house can help deliver faster diagnoses and more personalized patient care
From its beginning in 1993, the Randy W. Cooper Center for Breast Health Services at Piedmont Healthcare Augusta has aimed to provide a rapid-turnaround screening process for breast cancer patients with the goal of speeding up the imaging and biopsy processing time to help get results for patients sooner.

A streamlined user experience
High-quality staining with best-in-class turnaround time and first pass rates, allowing pathologists to confidently deliver results on first read.
- Innovative probe design
- Anti-hapten detection kits
- Enhanced target retrieval system

VENTANA HER2 Dual ISH demonstrated clinically meaningful first pass rates
The first pass rate for the VENTANA HER2 Dual ISH DNA Probe Cocktail assay on 40 breast samples fixed within the ASCO CAP guidelines (10% NBF for 6 to 72 hours) was 97.5% (87.1 – 99.6) on BenchMark ULTRA instruments. Specificity on the same 40 breast samples with negative control reagent was 100% (91.2 – 100) on BenchMark ULTRA instruments.1

Robust and reproducible staining, giving clear, confident reads
Detection chemistry with anti-hapten technology results in unparalleled signal intensity without increased background.
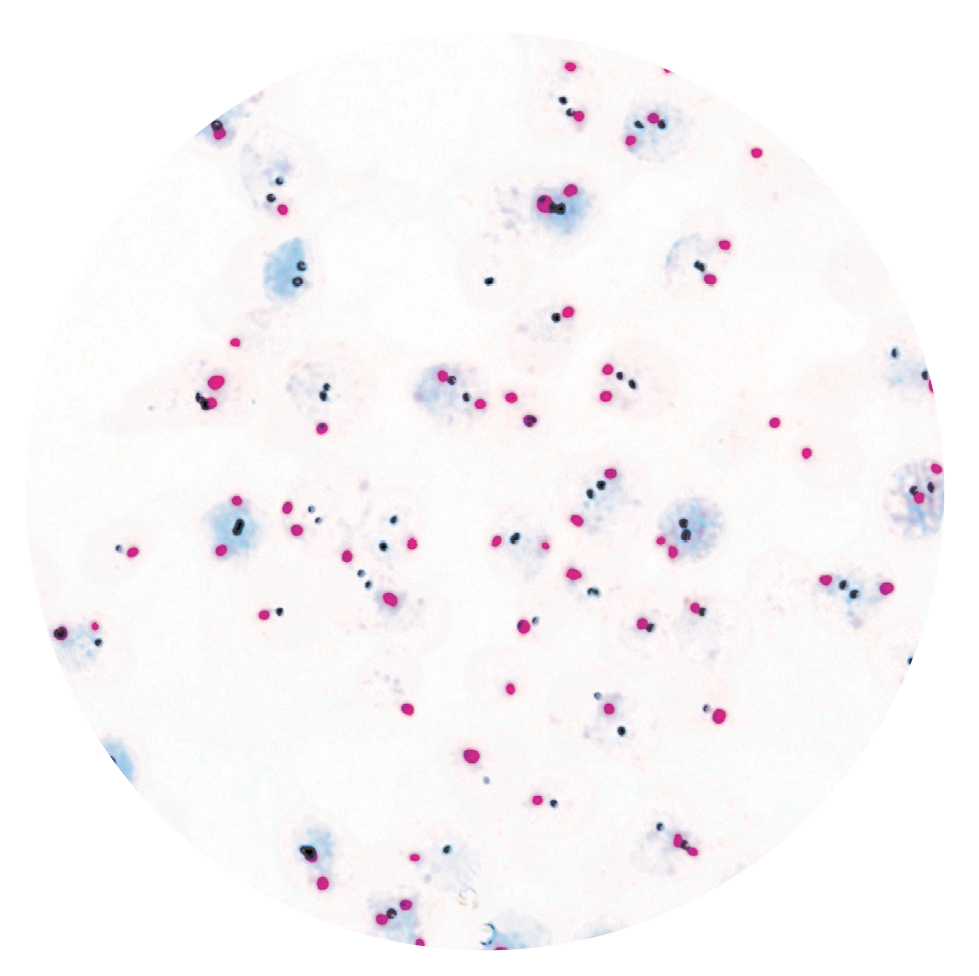
Breast carcinoma, 60X, Single copy HER2, nonamplified
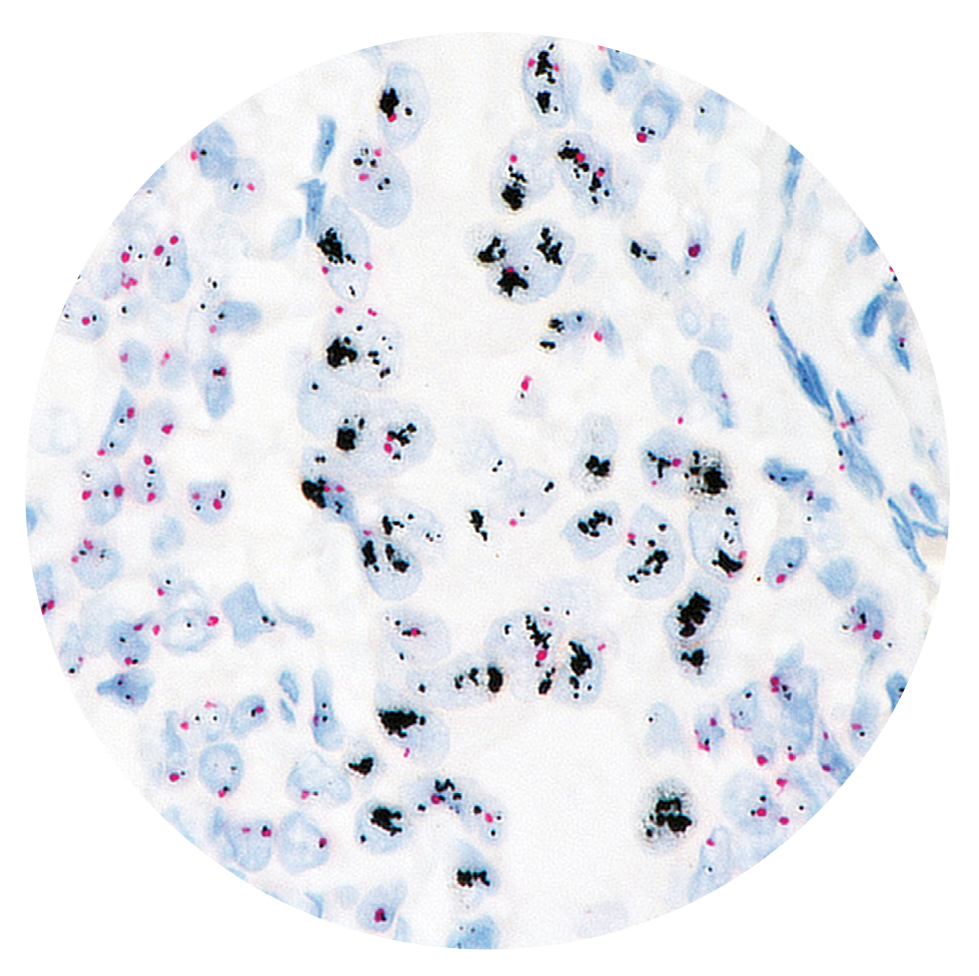
Breast carcinoma, 60X, HER2 clusters, amplified
Faster results with brightfield microscopy
The VENTANA HER2 Dual ISH assay is easily interpreted using brightfield microscopy,2 which has proven concordance with fluorescence in situ hybridization (FISH),1 enabling every lab the ability to run testing in-house that allows for faster results to the oncologist and their patient.
To evaluate the clinical sensitivity and specificity of the VENTANA HER2 Dual ISH DNA Probe Cocktail assay in determination of HER2 gene status in breast carcinoma, a multi-site method comparison study was performed using the Abbott/Vysis PathVysion HER-2 FISH Kit as the comparator device. Approximately 600 individual breast cancer cases were stained in 3 central laboratories.1

Why brightfield is better:
- No need for fluorescent microscope/oil and darkroom
- Fits into pathologist’s regular workflow at brightfield scope
- Can be read alongside/at same time as H&E and other breast panel markers on the same case for easy comparison and correlation of findings
- No interference from tissue autofluorescence or tissue marking dyes
- Produces archivable results
- Signals do not fade over time

Aligned with multiple professional guidelines
VENTANA HER2 Dual ISH DNA Probe Cocktail assay is indicated as an aid in the assessment of patients for whom HERCEPTIN® (trastuzumab) is being considered.
Multiple guidelines, including NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)3 and American Society of Clinical Oncology/College of American Pathologists (ASCO-CAP),4 recommend the evaluation of human epidermal growth factor receptor 2 (HER2) protein expression in breast cancer.

Educational Resources
Product Overview
Listen to a brief presentation from Roche pathologist Michael Lynch, MD, as he provides an overview of the new VENTANA HER2 Dual ISH assay.
Scoring the VENTANA HER2 Dual ISH Assay
In this short video, Roche pathologist, Michael Lynch, MD reviews the scoring method for the VENTANA HER2 Dual ISH assay as well as discusses scoring challenges and potential pitfalls.
INFORM HER2 Dual ISH vs. VENTANA HER2 Dual ISH
This video walks through the design improvements to the new VENTANA HER2 Dual ISH assay and reviews comparison slides to its predecessor , INFORM HER2 Dual ISH assay.
Understanding the Differences Between FISH and CISH Assays
Roche pathologist, Michael Lynch, M.D., discusses the differences between fluorescent in situ hybridization (FISH) and chromogenic in situ hybridization (CISH) and the practical implications to the laboratory.
Pathology Lab product catalog
View our Pathology Lab product catalog to see our complete portfolio, including the many ways Roche supports customers.
References
- Ventana Product Document Library. Package Insert, VENTANA HER2 Dual ISH DNA Probe Cocktail.
- Ventana Product Document Library. Interpretation Guide for VENTANA HER2 Dual ISH DNA Probe Cocktail assay; Staining for Breast Carcinoma.
- Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, Bilous M, Ellis IO, Fitzgibbons P, Hanna W, Jenkins RB, Press MF, Spears PA, Vance GH, Viale G, McShane LM, Dowsett M. J Clin Oncol. 2018 Jul 10;36(20):2105-2122.
- NCCN Guideline for Invasive Breast Cancer, Version 5.2020. NCCN Clinical Practice Guidelines in Oncology Breast Cancer. NCCN.org.
- Middleton LP, Price KM, Puig P, et al. Implementation of American Society of Clinical Oncology/College of American Pathologists HER2 Guideline Recommendations in a tertiary care facility increases HER2 immunohistochemistry and fluorescence in situ hybridisation concordance and decreases the number of inconclusive cases. Arch Pathol Lab Med. 2009;133(5):775-780.
- Khoury T, Sait S, Hwang H, Chandrasekhar R, et al. Delay to formalin fixation effect on breast biomarkers. Mod Pathol. 2009;22(11):1457-1467.
Cornerstone Diagnostics Assays: Helping You Deliver Personalized Healthcare

Committed to helping you deliver personalized healthcare
Our mission is to improve the lives of all patients afflicted with cancer. By empowering pathologists with the highest quality, innovative tools and personalized diagnostics, we ensure timely and accurate diagnoses, and subsequently, better patient care.
Treatment isn’t one-size-fits-all. Bridging the gap between generic and personalized treatment, we’re steadfast in our commitment to accelerate the development of new assays with the power to improve and extend patients’ lives.
World-class antibodies to stratify breast cancer

CA-125 (OC125) Mouse Monoclonal Antibody
Ordering Number: 05267269001
Catalog Number: 760-2610
Quantity: 50 tests
Controls: Ovarian Carcinoma
Localization: Membranous, Cytoplasmic

Calponin-1 (EP798Y) Rabbit Monoclonal Antibody
Ordering Number: 05435684001
Catalog Number: 760-4376
Quantity: 50 tests
Controls: Appendix
Localization: Cytoplasmic

E-cadherin (36) Mouse Monoclonal Primary Antibody, VENTANA
Ordering Number: 05905290001
Catalog Number: 790-4497
Quantity: 50 tests
Controls: Ductal Breast Carcinoma
Localization: Membranous

E-cadherin (EP700Y) Antibody
Ordering Number: 05973872001
Catalog Number: 760-4440
Quantity: 50 tests
Controls: Breast, Lung Adenocarcinoma, Pancreas
Localization: Membranous

Estrogen Receptor (ER) (SP1) Rabbit Monoclonal Primary Antibody, CONFIRM
Ordering Number: 05278406001, 05278414001
Catalog Number: 790-4324, 790-4325
Quantity: 50 tests, 250 tests
Controls: Breast
Localization: Nuclear

GATA3 (L50-823) Mouse Monoclonal Primary Antibody
Ordering Number: 07107749001
Catalog Number: 760-4897
Quantity: 50 tests
Controls: Ductal Carcinoma in situ
Localization: Nuclear

GCDFP-15 (EP1582Y) Rabbit Monoclonal Antibody
Ordering Number: 05463530001
Catalog Number: 760-4386
Quantity: 50 tests
Controls: Breast, Breast Carcinoma
Localization: Cytoplasmic

GLIAL Fibrillary Acidic Protein (EP672Y) Rabbit Monoclonal Antibody
Ordering Number: 05269784001
Catalog Number: 760-4345
Quantity: 50 tests
Controls: Brain
Localization: Cytoplasmic

Growth Hormone (polyclonal)
Ordering Number: 05268257001
Catalog Number: 760-2804
Quantity: 50 tests
Controls: Normal Pituitary
Localization: Cytoplasmic

Ki-67 (30-9) Rabbit Monoclonal Primary Antibody, CONFIRM
Ordering Number: 05278384001
Catalog Number: 790-4286
Quantity: 50 tests
Controls: Lymph Node, Tonsil
Localization: Nuclear

P53 (BP53-11) Primary Antibody
Ordering Number: 05267102001
Catalog Number: 760-2542
Quantity: 50 tests
Controls: Colon Adenocarcinoma
Localization: Nuclear

P53 (DO-7) Primary Antibody, CONFIRM
Ordering Number: 05278775001
Catalog Number: 800-2912
Quantity: 50 tests
Controls: Colon Adenocarcinoma
Localization: Nuclear

P57 (Kp10) Mouse Monoclonal Primary Antibody
Ordering Number: 06523897001
Catalog Number: 760-4617
Quantity: 50 tests
Controls: Placenta
Localization: Nuclear

P63 (4A4) Mouse Monoclonal Primary Antibody, VENTANA
Ordering Number: 05867061001
Catalog Number: 790-4509
Quantity: 50 tests
Controls: Prostate, Tonsil
Localization: Nuclear

P120 CATENIN (98) Mouse Monoclonal Primary Antibody, VENTANA
Ordering Number: 05867088001
Catalog Number: 790-4517
Quantity: 50 tests
Controls: Normal Ducts of the Breast
Localization: Membranous (ductal), Cytoplasmic (lobular)

PAX8 (MRQ-50) Mouse Monoclonal Primary Antibody
Ordering Number: 08008540001
Catalog Number: 741-4860
Quantity: 50 tests
Controls: Thyroid Carcinoma, Ovarian carcinoma (non-mucinous carcinoma)
Localization: Nuclear

PLAP (NB10)
Ordering Number: 05267757001
Catalog Number: 760-2664
Quantity: 50 tests
Controls: Placenta
Localization: Cytoplasmic

Progesterone Receptor (PR) (1E2) Rabbit Monoclonal Primary Antibody
Ordering Number: 05277990001, 05278392001
Catalog Number: 790-2223, 790-4296
Quantity: 50 tests, 250 tests
Controls: Breast
Localization: Nuclear

PTEN (SP218) Rabbit Monoclonal Primary Antibody
Ordering Number: 07970200001
Catalog Number: 790-5097
Quantity: 50 tests
Controls: Pancreatic Islet Cells
Localization: Cytoplasmic and/or Nuclear

Topoisomerase IIα (JS5B4) Rabbit Monoclonal Primary Antibody
Ordering Number: 05479339001
Catalog Number: 790-4371
Quantity: 50 tests
Controls: Spleen, Tonsil
Localization: Nuclear

Actin, Smooth Muscle (1A4) Mouse Monoclonal Antibody
Ordering Number: 05268303001
Catalog Number: 760-2833
Quantity: 50 tests
Controls: Appendix, Uterus
Localization: Cytoplasmic

Caldesmon (E89) Rabbit Monoclonal Primary Antibody
Ordering Number: 05463459001
Catalog Number: 760-4375
Quantity: 50 tests
Controls: Esophagus, Smooth Muscle from Bowel, Uterus
Localization: Cytoplasmic

Cytokeratin (35betaH11) Mouse Monoclonal Primary Antibody
Ordering Number: 05267471001
Catalog Number: 760-2637
Quantity: 50 tests
Controls: Prostate
Localization: Cytoplasmic
Pathology Lab product catalog
View our Pathology Lab product catalog to see our complete portfolio, including the many ways Roche supports customers.
Predictive Diagnostic Pipeline

Investing in the future means investing in all of our futures
Breast cancer has a profound impact on the diagnosed patient, their family, their friends, and everyone in their lives. We know that we have to look to the future and keep innovating every day because of this impact.
We have an active number of products in development with the ultimate goal of bringing these solutions to market, to our customers, and, most importantly, to the patients that need them the most.
What’s in the pipeline?
A mix of new assays and indications, solutions to support further automation in labs, as well as digital and data solutions are all part of our investment in research and development. These are subject to change based on development and regulatory requirements.
Building a robust pipeline of predictive diagnostics
Continued expansion in medical value across 12 disease areas

*Biomarkers shown represent areas of interest for research and development. It is not a complete list.
Want even more details about what we’re up to for the future and how it could be of benefit to you?
Let’s talk. No matter the role you have within your organization, we’d welcome a conversation and will answer any questions you may have.
Pathology Lab product catalog
View our Pathology Lab product catalog to see our complete portfolio, including the many ways Roche supports customers.

Here’s how you can connect with us:
Visit our Contact us and support page
Visit our What's New with Roche Pathology Lab page